
BRINSUPRI was studied in a clinical trial involving more than 1700 patients with non-cystic fibrosis bronchiectasis (NCFB)1
ASPEN was a Phase 3 placebo-controlled trial1,2

The ASPEN study was an international, multicenter, randomized, double-blind, parallel-group, placebo-controlled Phase 3 clinical trial. Patients were 12 to 85 years of age (41 adolescents and 1680 adults) and received 1 of 2 doses of BRINSUPRI (10 mg: n=583; 25 mg: n=575) or placebo (n=563), administered once daily for 52 weeks.1,2
Patients in all arms were permitted to continue using their existing concomitant therapy.2,3
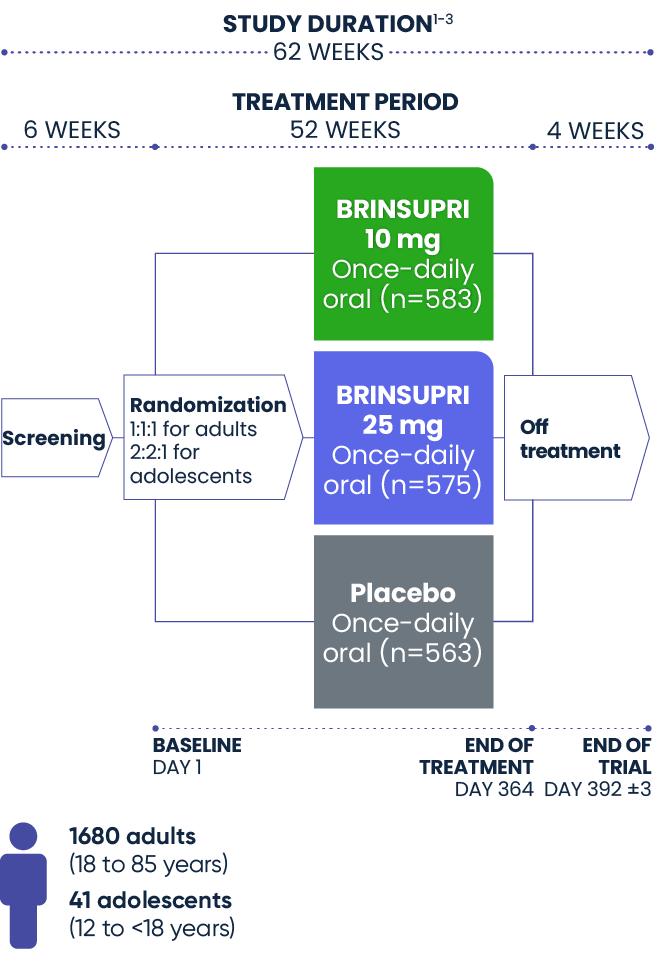
All patients enrolled in ASPEN had a clinical history of confirmed NCFB by chest computed tomography (CT). Adult patients had at least 2 documented pulmonary exacerbations prior to screening in the prior 12 months. Adolescent patients had at least 1 pulmonary exacerbation in the prior 12 months.1,2
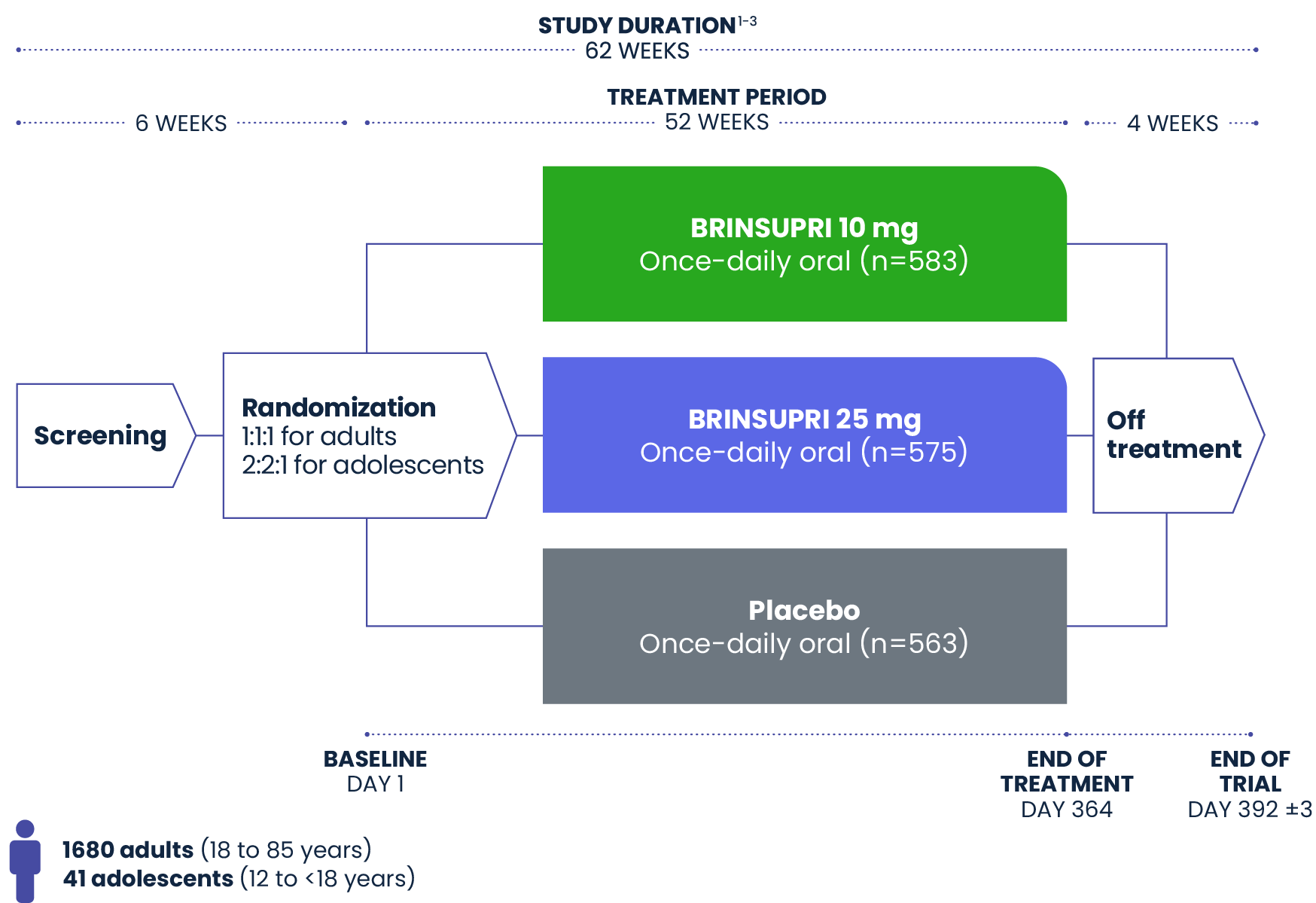
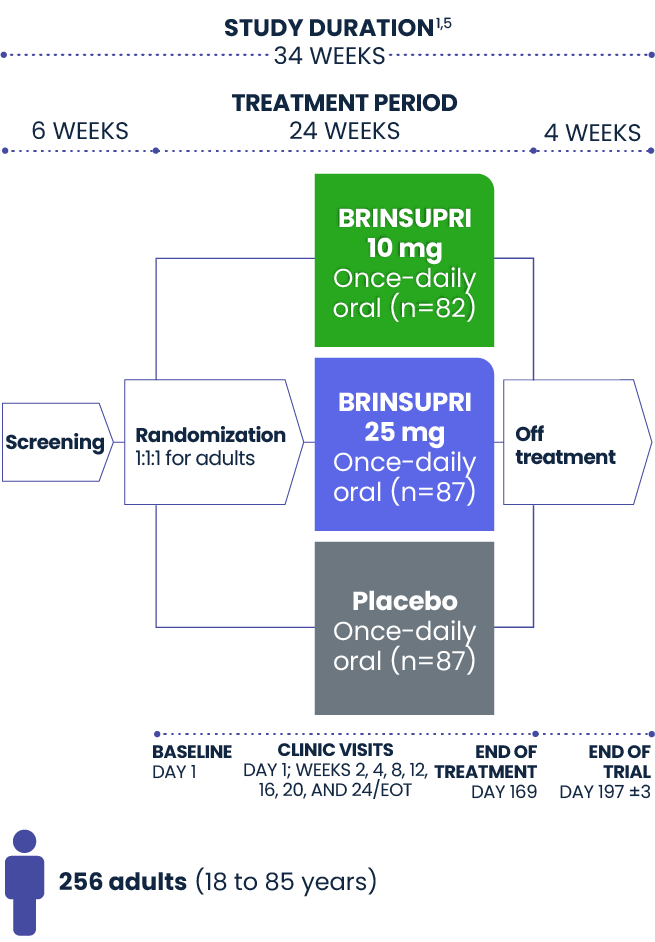
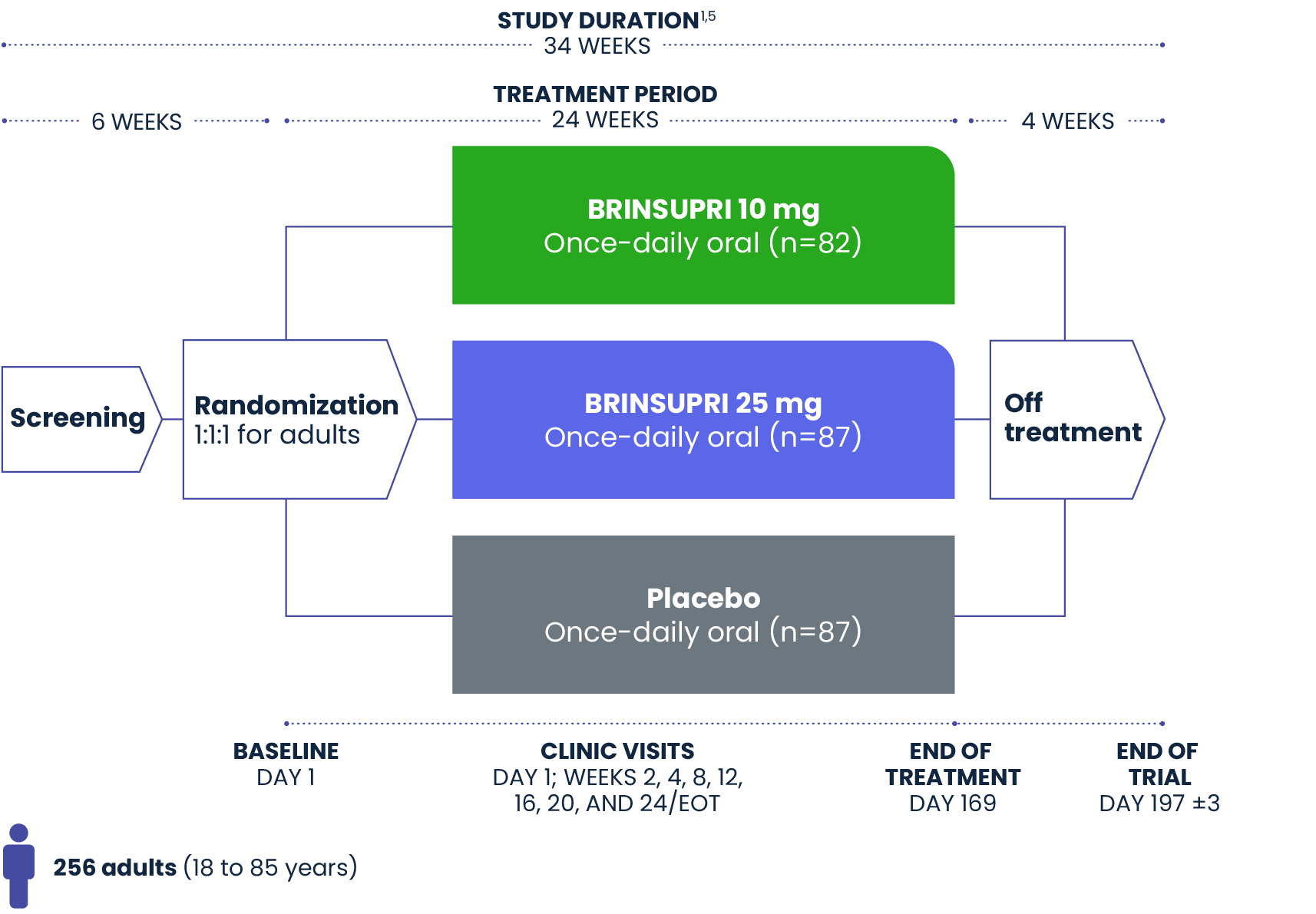
WILLOW was a Phase 2 placebo-controlled trial1,4
WILLOW was a randomized, double-blind, placebo-controlled, parallel-group, multicenter, multinational Phase 2 clinical trial with 256 patients. Adults with NCFB received either BRINSUPRI (10 mg, 25 mg) or placebo once daily for 24 weeks.1,4
Demographic and baseline characteristics of patients in ASPEN and WILLOW1,2,6
Patient characteristics in ASPEN were representative of real-world populations of patients with bronchiectasis.
ASPEN
(N=1721)
n (%)
WILLOW
(N=256)
n (%)
Pseudomonas aeruginosa
Primary endpoint of ASPEN1:
Annualized rate of pulmonary exacerbations
Secondary endpoints (hierarchical) of ASPEN2:
Time to first exacerbation
Percentage of patients who remained exacerbation free at Week 52
Change from baseline in post-BD FEV1 at Week 52
Annualized rate of severe pulmonary exacerbations
Primary endpoint of WILLOW1:
Time to first exacerbation over 24 weeks
BRINSUPRI was proven to reduce the risk of exacerbations1
BD=bronchodilator; EOT=end of treatment; FEV1=forced expiratory volume in 1 second; PEx=pulmonary exacerbation; ppFEV1=percent predicted forced expiratory volume in 1 second; SD=standard deviation.